Vermont Business Magazine The Vermont Department of Health reported June 28 that COVID-19 cases and hospitalizations are still considered "Low." Total cases for the week were up slightly, while hospitalizations declined. Levels in June remain near their lowest since a surge in cases that began last August. Deaths attributed to COVID-19 stand at 683. There have been 11 deaths in June attributed to COVID so far after 32 in May. May saw an increase in fatalities from April and March. June is on pace to have the fewest COVID fatalities since last July (2).
Vermonters are reminded that all state COVID testing sites closed as of June 25. PCR and take home tests will be available through doctors' offices, pharmacies and via mail from the federal government. See more information here: https://www.healthvermont.gov/covid-19/testing
Report Timeframe: June 19 to June 25, 2022
Statewide community levels: Low. The rate of new COVID-19 cases per 100,000 Vermonters is below 200. New COVID-19 admissions are below 10 per 100,000 Vermonters per day, and the percent of staffed hospital beds occupied by COVID-19 is below 10%.
• New COVID-19 cases, last 7 days: 104.65 per 100K (last week 103.21 per 100K)
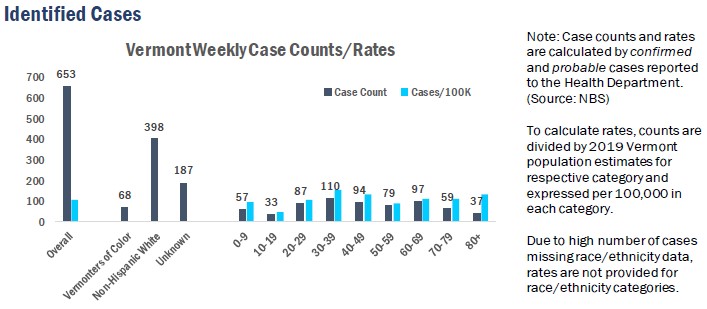
o Weekly Case Count: 653 (increase of seven total cases from last week)
• New hospital admissions of patients with COVID-19, last 7 days: 5.29 per 100K (last week 6.73 per 100K
o 33 total new admissions with COVID-19 (decrease of nine from previous week)
• Percent of staffed inpatient beds occupied by patients with COVID-19 (7-day average): 1.47%
(decrease from last week's 2.13%)
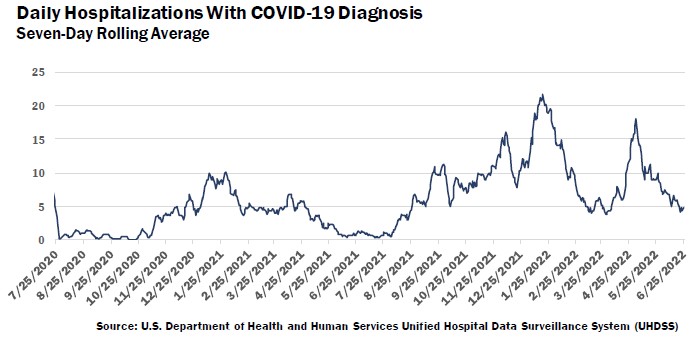
The seven-day rolling average of hospital patients admitted with a laboratory-confirmed COVID-19 infection peaked in January 2022 and increased again throughout April and into early May. The average has since trended downward and is currently under five such hospitalizations a day for the first time since early April 2022. The number is the daily average of the previous seven days; for
example, the value for May 28 is the daily average for the days of May 21 through May 27.
Syndromic Surveillance
Vermont is using the Electronic Surveillance System for the Early Notification of Community-based Epidemics (ESSENCE), which provides all individual emergency department visits from participating emergency departments1 to identify Emergency Department visits for COVID-like illness (CLI).
During this reporting period under 3% of emergency visits in participating emergency departments have included CLI. This is the lowest proportion since March of 2022, though slightly higher than the same calendar dates in the previous two years.
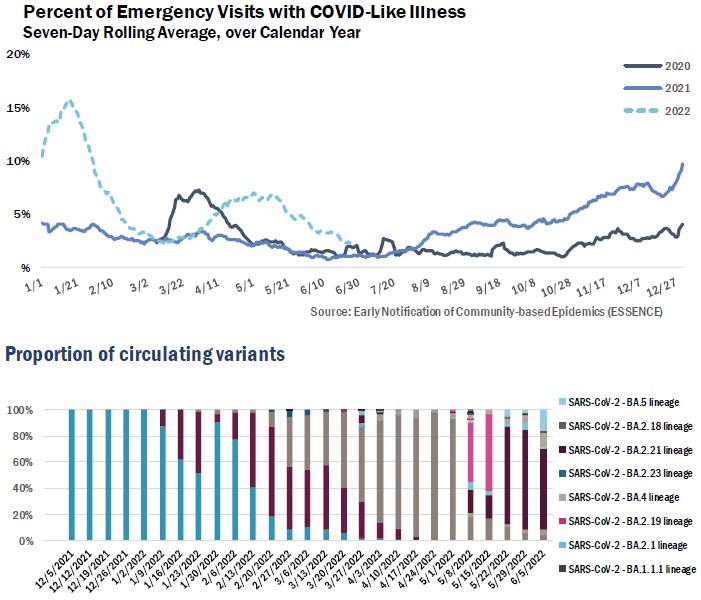
Among the most recent sequenced samples collected in Vermont (the week of 6/5), BA.4 (11%) and BA.5 (16%) comprised their largest virus proportion so far. The majority remained BA.2 and its subvariants. All sequenced samples remain Omicron variants.
(Sources: Broad; Health Department Whole Genome Sequencing program)
1 All Vermont hospitals and two urgent care clinics are included in ESSENCE.
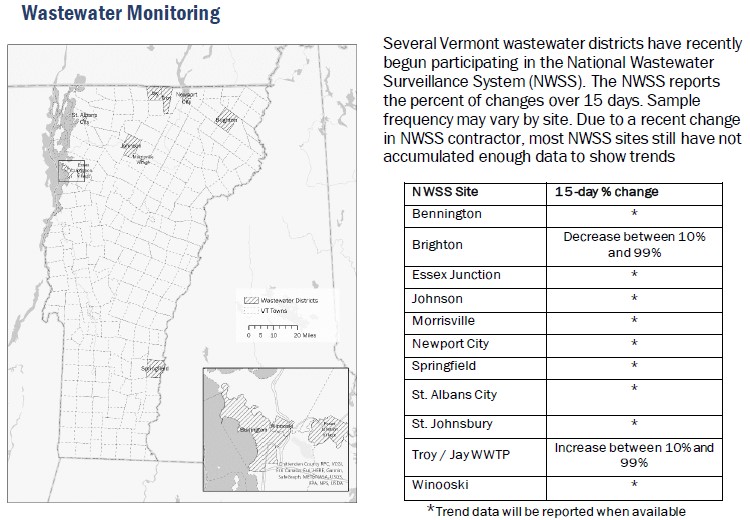
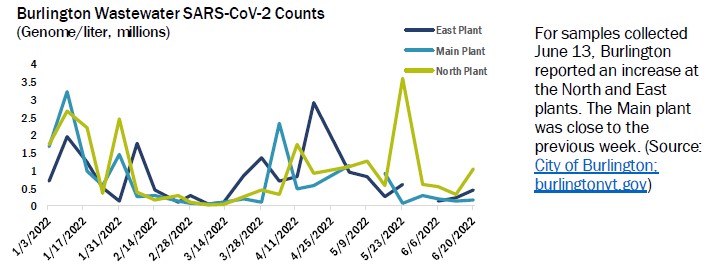
In addition to Vermont’s NWSS sites, the City of Burlington has been collecting samples in collaboration with the Health Department and research partners at the University of Vermont and at Dartmouth-Hitchcock Medical Center. Burlington has been collecting data since August 2020, and reports on the 24-hour viral concentration (as genomes per liter) of SARS-CoV-2 ribonucleic acid (RNA) collected at the city’s three wastewater plants.
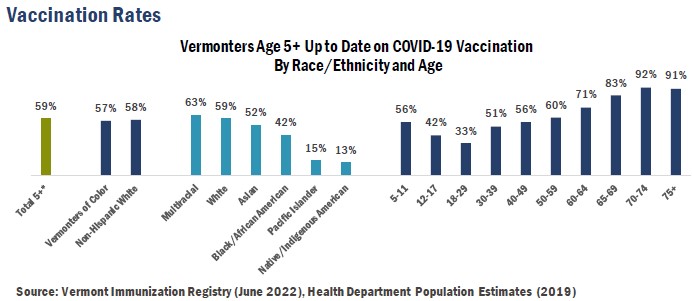
Note: Race/ethnicity information is missing for 4% of vaccinated individuals. Population denominators are from 2019 population estimates so percentages shown are an estimate which may vary from the true proportion in the population, particularly for smaller groups. “Up to date” means a person has received all recommended doses in their primary series of COVID-19 vaccine, and one booster dose when eligible.
COVID-19 vaccination rates for Vermonters who identify as Pacific Islanders or Native American, Indigenous, or First Nation have been substantially lower than rates for other Vermonters. In addition, the number of people in the Vermont Immunization Registry who identify as Pacific Islanders or Native American, Indigenous, or First Nation are much lower than our Vermont Department of Health population estimates. These findings could be due to one or more of the following:
1) Pacific Islanders and Native/Indigenous Americans are less likely to report their race.
2) Pacific Islanders and Native/Indigenous Americans are receiving fewer vaccinations.
3) Health Department population estimates are overestimating the true population.
4) Race and ethnicity are collected by providers in a way that does not align with how people identify.
COVID-19 Deaths
Vermont has the second fewest deaths per capita in the US (109 per 100,000), behind only Hawaii (105). Mississippi (420) and Arizona (418) have the highest rates.
As of June 29, 2022, there have been 1,016,809 COVID-19 related deaths in the United States (Brazil second most with 670,848) and 6,333,144 total worldwide (source: Johns Hopkins)..
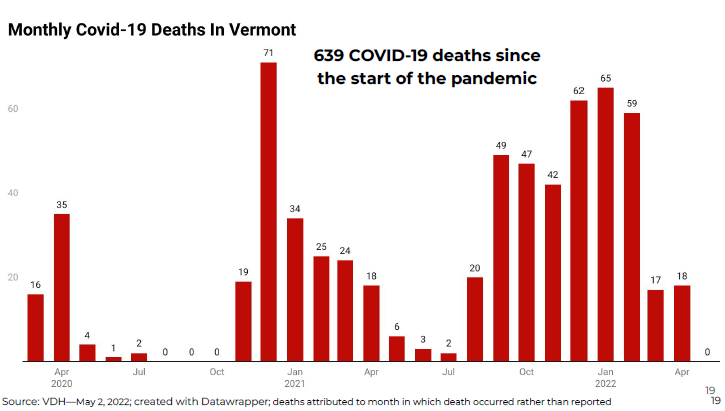
There were 49 COVID-19 related fatalities in Vermont in September 2021, and 47 deaths in October, which are the fifth- and sixth-worst months on record. There were 42 fatalities in November, 62 in December, and 65 in January 2022, 59 in February, 17 in March, 19 in April and 32 in May, as fatalities rose early in the month before falling off. There have been 11 deaths in June. The Delta variant caused a surge in COVID-related fatalities last fall and into the winter.
More than half of all deaths overall have been of Vermonters 80 or over.
While the highest concentration of deaths were from last September through February, December 2020 was the worst month with 71.
The VDH ceased publishing its daily dashboard in May.
Vermont Department of Health recommendations: Protect Yourself & Others CDC recommendations: COVID-19 by County | CDC
Source: VDH 6.28.2022 https://www.healthvermont.gov/covid-19