by Timothy McQuiston Vermont Business Magazine Vermont Auditor Doug Hoffer had praise for the progress made by Vermont Health Connect, the state’s health insurance marketplace, but also had several concerns, in an audit of VHC dated November 18. Among the concerns he has is: the lack of full implementation of enhancements; the software developer’s (Exeter) decision to no longer support a key component; a failure to follow protocol in contracting policy; and lingering security weaknesses.
 Hoffer said in the report: “The addition of automated change of circumstances and QHP (Qualified Health Plan) renewals are significant improvements to the VHC system’s functionality that should help alleviate customer dissatisfaction with the system.
Hoffer said in the report: “The addition of automated change of circumstances and QHP (Qualified Health Plan) renewals are significant improvements to the VHC system’s functionality that should help alleviate customer dissatisfaction with the system.
“However, other significant improvements to be implemented remain in order to fully comply with the Patient Protection and Affordable Care Act and Medicaid requirements, such as Medicaid renewals, SHOP, and Medicaid billing.
“The ability of the State to make changes to the VHC system has been made more difficult by Exeter Group’s decision not to support OneGate or provide the State with professional services to support the VHC system.
“In addition, while improvements have been made to VHC security, there continues to be high and moderate risk weaknesses to be remediated.
“As decisions are made about the future of VHC, it is important to consider both the current state of the system and its planned future state and the time and money it will take to achieve the final end result.”
RELATED:
Governor provides update on Vermont Health Connect open enrollment
In addition to the technical parts of VHC, he added:
“During the course of our audit we found that DVHA had authorized contractors to perform work in a manner that circumvented the State’s contracting policy. In particular, the State’s procurement policy, Bulletin 3.5, does not authorize or even mention the use of authorization to proceed letters. Bulletin 3.5 has mechanisms for state organizations to seek approval for exceptions to its requirements, but such approval was not obtained.”
Agency of Human Services Secretary Hal Cohen agreed with all of Hoffer's findings in his official response to the audit, saying in part:
"As your report accurately notes, Vermont Health Connect (VHC) has made significant improvements in several key area that were called for in Act 58. While we acknowledge that certain enhancements remain to be completed, and additional work is needed in order to further improve the functionality of the VHC system, I am confident that our dedicated VHC team will be successful in its efforts to complete those tasks.
“With VHC operational and open enrollment for the 2016 plan year going smoothly, it’s important to recognize and appreciate the efforts of the staff in helping to get us to this point.”
As for the specific corrective action regarding that “DVHA authorized Optum and Exeter Group to perform work using a document called an “authorization to proceed” letter that was not authorized by the State’s procurement policy (Bulletin 3.5) and had not been otherwise approved. In other cases, Optum and Archetype were performing work without benefit of any written agreements at all.
Hoffer recommended:
1. Immediately negotiate and sign contracts or contract amendments with Optum, Exeter Group, and Archetype for the work currently being performed without benefit of such documents.
2. Immediately stop the use of ATPs until such time as the Secretary of Administration has approved their use either through an approved contracting plan or waiver as called for in Bulletin 3.5.
To those recommendations, Cohen said in his response:
“Although DVHA had a different understanding at the time, the Department is now aware it should seek Secretary of Administration approval for (authorization to proceed agreements) … and will seek such approvals going forward.”
Governor Peter Shumlin said last spring that if the state failed to meet certain milestones then he would recommend to the Legislature that VHC be disbanded and the state should move to the federal exchange.
Earlier this week, he gave a promising status update to VHC that while acknowledging that work still needs to be done, significant progress, especially in customer satisfaction and automation, has been achieved.
“The number of Vermonters who are completely through the renewal process at this point is very encouraging,” Shumlin said. “This year is a totally different ballgame, and I am pleased with the progress that is being made.”
So far this open enrollment period, more than 18,000 individuals are completely through the renewal process, having had their 2016 plans confirmed with Vermont Health Connect’s payment processor and insurance carrier partners. It is expected that all customers will be processed into their 2016 plans by the end of November in time for their January invoice, which mails in early December. There are approximately 30,000 individuals currently enrolled in qualified health plans through Vermont Health Connect.
By way of comparison, the state is two months ahead of where it was last year when Vermont Health Connect did not reach 18,000 individuals completely through the renewal process until late January.
“I’m very appreciative to Vermonters for their patience through this process,” Shumlin said. “While we will continue to work to improve Vermont Health Connect, the time for talking about scrapping it and moving to the federal exchange is over. We should all come together to work to make our exchange a success.”
Hoffer's audit is entitled "VERMONT HEALTH CONNECT, Status of Planned Enhancements" and was sent to legislative leaders and relevant agency heads. Among his comments in the introduction he said: "The State deployed several software changes to the VHC system since the end of May 2015 that generally implemented the COC (Change of Circumstance) and QHP renewal processes called for in Act 58.
"Overall, the result of these changes appears positive in that customer complaints regarding the execution of their changes have been fewer and significant operational improvements have ensued. Nevertheless, the true test will come during the on-going open enrollment period (November 1, 2015 to January 31, 2016)."
Maintenance and Operations Processes
Figure 1 illustrates that the number of open maintenance and operations tickets began to increase in early June 2015, after the implementation of R1, and has remained at much higher levels than the four months prior to the deployment. Tickets are summarized in three categories: incidents, problems, and service requests. An incident is an unplanned interruption or reduction in the quality of an IT service. For example, a user may be unable to log in or an unexpected error may have occurred while processing a transaction. A problem is defined as an underlying root cause of one or more incidents or a defect introduced into the production environment by a software release. According to an Optum spreadsheet of problem tickets, about half of this type of open ticket (142 of 260 as of October 28, 2015) resulted from software releases deployed with uncorrected system defects (called a “leaked defect”). Examples of “leaked defect” problem tickets are anomalies on the customer portal or the system assigned a QHP to an individual who had obtained Medicare. Service requests are minor changes that are discretionary or non-discretionary.
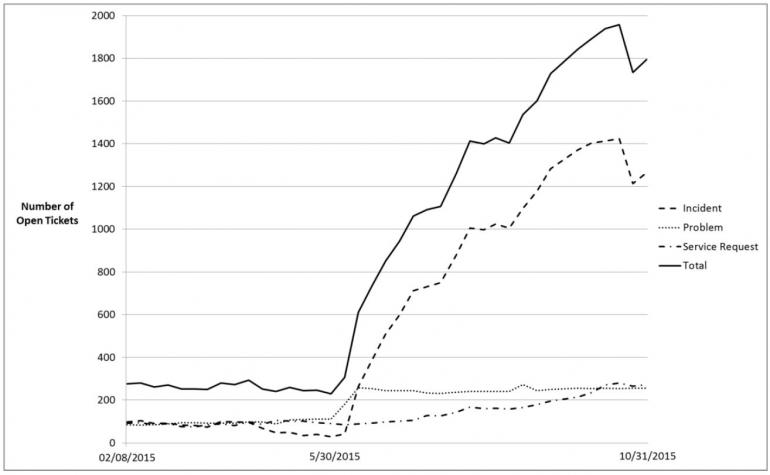 Figure 1: Number of Open Maintenance and Operations Tickets between February 8, 2015 and October 31, 2015, Based on Weekly Optum Summary Reports
Figure 1: Number of Open Maintenance and Operations Tickets between February 8, 2015 and October 31, 2015, Based on Weekly Optum Summary Reports