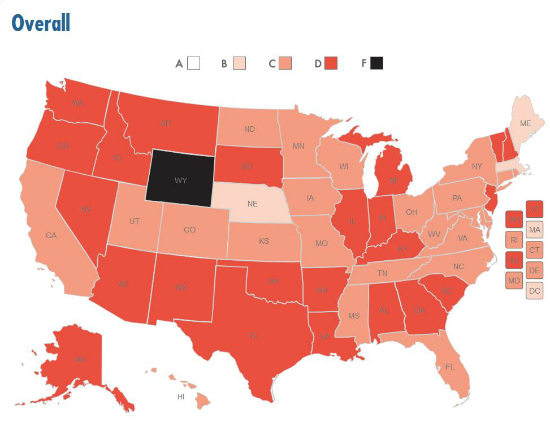
Vermont dropped to 33rd place in the nation with a D+ in the 2014 American College of Emergency Physicians’ (ACEP) state-by-state report card on America’s emergency care environment. A lack of statewide planning and policies in the category of Disaster Preparedness contributed to this drop. In 2009, Vermont received an overall C grade and ranked 21st in the nation.’ The US overall also dropped to D+.
Vermont’s Disaster Preparedness decline in both grade and rank ‘falling from 16th place with a B in 2009 to 40th place with an F ‘ are principally attributable to a lack of statewide policies and a low level of volunteer capacity compared with other states. The state has no provisions for patients dependent on dialysis or medication for chronic diseases. In addition, it lacks strike teams to provide assistance during disaster or mass casualty events and has no behavioral health professionals registered in the Emergency System for Advance Registration of Volunteer Health Professionals.
‘Vermont’s disaster preparedness efforts must rise to the gold standard set by Boston after the Marathon bombing,’ said Dr. Peter Weimersheimer, president of the Vermont Chapter of ACEP. ‘The memories of Hurricane Irene in 2011 are still fresh in peoples’ minds. This Report Card should spur policymakers to ensure that every medical provider in our state is ready for anything at any time so that history doesn’t repeat itself.’
Vermont’s best grade, a 13th place ranking and a B in Public Health and Injury Prevention, reflects high immunization rates and one of the lowest infant mortality rates in the country. The state also has relatively low levels of obesity.
Vermont received a D in the category of Access to Emergency Care. Contributing to this grade include a declining pool of hospitals, emergency departments, inpatient beds and psychiatric care beds. According to the Report Card, to improve this grade, Vermont must increase its hospital capacity and reduce the long wait times (295 minutes) in emergency departments, which can lead to poor patient outcomes.
‘Patients are waiting nearly 5 hours in our ERs for care,’ said Dr. Weimersheimer. ‘The best medical care in the world won’t help you if you can’t get to it in a timely manner.’
The state’s 25th place ranking and C+ for Quality and Safety Environment are a marked improved from its 33rd place ranking and C- in 2009. Vermont continues to fund an emergency medical services medical director and has implemented stroke and heart attack systems of care. The state leads the nation in the time it takes to transfer patients with chest pain to an appropriate facility. It should continue to improve on its performance in this area by developing destination policies for stroke and heart attack patients.
Vermont also improved its grade for Medical Liability Environment from an F to a D-, although there is still significant room for improvement. The state lacks any expert witness rules requiring experts to practice in the same specialty as the defendant or to be licensed to practice in the state. To improve this grade, Vermont must support providers of federally mandated care delivered in emergency departments by offering additional liability protections that recognize the risk entailed in providing this care and requiring clear and convincing evidence of negligence in medical liability cases.
‘America’s Emergency Care Environment: A State-by-State Report Card ‘ 2014’ evaluates conditions under which emergency care is being delivered, not the quality of care provided by hospitals and emergency providers. It has 136 measures in five categories: access to emergency care (30 percent of the grade), quality and patient safety (20 percent), medical liability environment (20 percent), public health and injury prevention (15 percent) and disaster preparedness (15 percent). While America earned an overall mediocre grade of C- on the Report Card issued in 2009, this year the country received a near-failing grade of D+.
ACEP is the national medical specialty society representing emergency medicine. ACEP is committed to advancing emergency care through continuing education, research and public education. Headquartered in Dallas, Texas, ACEP has 53 chapters representing each state, as well as Puerto Rico and the District of Columbia. A Government Services Chapter represents emergency physicians employed by military branches and other government agencies. - See more at: http://www.emreportcard.org/Content.aspx?id=514#sthash.WqH6hdJO.dpuf.
Vermont's overall score has declined, largely due to a lack of statewide planning and policies in Disaster Preparedness, as well as declining hospital capacity. The state continues, however, to invest in and improve its Quality and Patient Safety Environment.
VERMONT REPORT
Strengths
Vermont has improved its Quality and Patient Safety Environment by supporting measures to improve care and emergency response capabilities statewide. The state has continued funding for an emergency medical services (EMS) medical director, as well as quality improvement within the EMS system, and has worked to implement stroke and ST-elevation myocardial infarction (STEMI) systems of care. Vermont leads the nation in the time that it takes to transfer patients with chest pain or acute coronary intervention to another facility (28 minutes).
Vermont continues to fare well in Public Health and Injury Prevention, with high immunization rates and moderate health risk factors. The state boasts high vaccination rates for older adults, with 65.4% having received an annual influenza vaccination and 74.3% having ever received the pneumococcal vaccine. Vermont also has one of the lowest infant mortality rates (4.2 deaths per 1,000 live births) and below-average proportions of adults and children who are obese (25.4% and 11.3%, respectively).
In Access to Emergency Care, Vermont performs exceptionally in reducing financial barriers to care, boasting some of the highest rates of health insurance coverage for adults and children in the nation. The state has relatively high Medicaid fee levels for office visits (117.1% of the national average). Vermont also has adequate access to providers, including primary care providers, many types of specialists, and emergency physicians.
Challenges
Vermont fares poorly overall in Access to Emergency Care because of the lack of specialty centers and declining hospital capacity. The state has no accredited chest pain centers and ranks second to last for the number of pediatric specialty centers (1.6 per 1 million people). Only 78.5% of the population is within 60 minutes of a level I or II trauma center, compared to an average of 82.1% nationally. Vermont has seen an overall decline since the previous Report Card in staffed inpatient beds, emergency departments (ED), and psychiatric care beds and an increase in the hospital occupancy rate. As such, the state has higher-than-average ED wait times: 295 minutes from ED arrival to ED departure for admitted patients.
While Vermont's Medical Liability Environment ranking has improved slightly since the 2009 Report Card, this is due only to minor improvements and the addition of apology inadmissibility laws, which is the only measured reform that Vermont is credited with having. The state lacks any expert witness rules requiring experts to practice in the same specialty as the defendant or to be licensed to practice in the state, rules that can prevent unfounded cases from proceeding. The state has also failed to enact special liability protections for care mandated by the Emergency Medical Treatment and Labor Act (EMTALA). Vermont has seen an increase in its average malpractice award payment yet has no reforms in place that would help to rein in excessive payments.
Vermont's Disaster Preparedness grade declined significantly, due in part to the addition of new indicators and because of a lack of statewide policies and a low level of volunteer capacity compared to other states. Vermont's medical response plan lacks provisions for patients dependent on dialysis or medication for chronic diseases. It has no mutual aid agreements in place with behavioral health providers to provide services during a disaster and no behavioral health professionals registered in the Emergency System for Advance Registration of Volunteer Health Professionals. Vermont also lacks strike teams or medical assistance teams to provide assistance during a disaster or mass casualty event.
Recommendations
Vermont policymakers must seriously consider the impact of such a poor Medical Liability Environment on both providers and patients. While the state has an adequate supply of many types of providers, day in and day out, emergency physicians and on-call specialists provide care to high-risk patients and must make quick decisions with little or no knowledge of their medical history. The state must support providers of EMTALA-mandated care by offering additional liability protections that recognize those risks and that at least require clear and convincing evidence of negligence in medical liability cases. Vermont could also consider pretrial screening panels and requiring that expert witnesses be of the same specialty as the defendant.
Vermont should continue to build upon existing improvements to the Quality and Patient Safety Environment by developing destination policies for stroke and STEMI patients that would allow EMS providers to bypass local hospitals for medical specialty centers when appropriate. Finally, Vermont must work with stakeholders to increase its hospital capacity and reduce the long ED wait times, which can lead to poor patient outcomes.
More Information
Complete National Report’(PDF)
Vermont State Detail Report’(PDF)
- See more at: http://www.emreportcard.org/Vermont/#sthash.JDhmeeew.dpuf